|
Dr Melanie Ann Liebenberg
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
CURRENT
POSTS 2013
Dr
Liebenberg trained at
the University of Stellenbosch,
South Africa where she obtained her MBChB
in 1986. DCH 1995, FCP(Paed)SA 1997 (University of Cape Town, South Africa).
She was admitted to the UK Specialist register in 1999 via equivalence route.
In the past she has been called by the Crown as a specialist witness. Title: Dr Clinical Excellence Award
Note: The Lushington Clinic LLP is limited liability partnership registered in England & Wales under registration number OC308529.
EASTBOURNE DGH IN THE NEWS
The relatives of nine patients who were treated at Queen’s Hospital in Romford, Essex and nine who were treated at Eastbourne District General Hospital, East Sussex, have instructed lawyers to pursue their claims, according to Radio 4’s Today programme.
Getting yourself admitted to hospital is just as worrying these days because you may go in for something minor and not come out except in a hearse. The hospital will be sure to profit from your visit in every way - before you die. Car park charges is another 'rip-off' for debate.
JUNE 2015 USA - HOW EASY IS IT TO GAIN A CONVICTION BY STATING FALSEHOODS AS FACTS
On 3 April 1981
Kirk Odom was walking near his home in
Washington DC when he was stopped by a police officer. It was just a random passing in the street. Odom had done nothing, been nowhere. He was an unexceptional 18-year-old trying to raise his infant daughter Katrice who was then less than a year old.
JAILED FOR 22 YEARS ON BOGUS HAIR EVIDENCE
The testimony, proudly invoking the certainties of science, did its job: the verdict came in guilty. On the basis of that single hair Kirk Odom was to spend the next 22 years in prison and a further nine living the half-life of a paroled sex offender.
How is that different from the case below? Apart from the fact that Melanie Liebenberg misled the Jury as to anatomical evidence, rather than the matching of a hair - It isn't. Dr Liebenberg used out of date medical evidence to seal a wrongful conviction, the FBI used outdated anatomical evidence. Is it not time that the UK did the research to not only convict those guilty of offences, but also to protect those falsely accused of crimes. Ref: The Guardian, Ed Pilkington
TEN YEARS AND COUNTING - Oh dear me. Dr Liebenberg was an expert witness in the case below alleging rape. Sometimes experts think that are doing the right thing by not following the correct procedures and not telling it like it is with new guidance about to be published. The girl in this claim was examined in 2006 using old thinking to compile a report. The trial below was held in February of 2008. In March of 2008 the above guidance was issued. In this guidance, the correct procedure for examining claimants is spelled out. We wonder if dear old Melanie had seen this document in draft form before giving her evidence. If so, that would compound the misdirection that the jury were given and that would be fraud. If not, then it is a curious coincidence that Liebenberg failed to conduct her examination in a manner that would benefit the defence, but would most assuredly disadvantage the defendant. As reporters, we have seen the good doctor's report from 2006. In this report Liebenberg says that Claimant H was: "Tightly closed and could not be opened with labial traction." Here she was referring to the girl's hymen. We have also read the above Guidance, and in those pages it is clear that if a girl is interfered with more than once, her hymen will not be tightly closed. There is a reliable method of measuring virginity, using the distance from the hymen to the vaginal wall. The instrument used is called a Colposcope. In this case the examiner did not obtain the adolescent's medical history, so did not know that she had a congenital birth defect, which fortunately she could not have attributed to the defendant.
It is important when constructing a jigsaw puzzle, to have all the pieces. For example, the examiner did not know that there had been heated exchanges between the defendant and her mother and that he'd recently called off an engagement. The girl was also a gymnast and previously rode horses. None of the Class 3-4 signs were present, as one might have expected if as claimed, the girl had been regularly penetrated. The trial judge told the jury this might have been on 40 occasions - thus virtually instructing the jury to convict.
Dr Liebenberg failed to mention to the jury that none of the expected lacerations, transections and/or healed scars to the fossa or posterior fourchette - or angular clefts or tears, or labial adhesions of the hymen were present. She might have mentioned that the absence of any and all of these signs, given the claimed regularity of abuse, was not consistent with the allegations. But stands to be considered as part of a conspiracy to pervert the course of justice. Dr Liebenberg could have mentioned that had any of these signs been in evidence, that would have been either definitive proof of sexual abuse or at best highly suspicious circumstances. But, as we stress - none of these were present and the jury had a right to know that before sending a man to prison.
This evidence does not stand alone. There is a diary that casts doubt as to opportunity which the girl's mother hid in her loft so that the police would not find it. On the stand under duress the girl's mother revealed its existence, but then she knew that the defence would not have time to cross reference the dates in it with the girl's testimony. Judge Cedric Joseph then wrongly told the jury that this diary was the defendants - and still the CCRC turn a blind eye.
Compounding that crafting of the evidence, Gordon Staker, James Hookway and Jo Pinyoun failed to either secure or mention the existence of the defendant's diaries, wherein the claimant's mother, a community psychiatric nurse had written in her own hand that the accused should not forget Valentines Day.
The plot thickens where solicitor Timothy Stirmey and barrister Julian Dale were provided with the diary entries, the accused pointing out that the entries were written in his diaries by the mother of the claimant, but his legal team failed to use this evidence in rebuttal of the claim that a Valentines Day Card sent to the claimant was in respect of the insistence of the claimant's mother to cheer her daughter up. This was because the claimant did not have a boyfriend and was not popular at school with the opposite sex.
What possible excuse could Stirmey and Dale give for not putting this vital information before the Jury? We can only think of one thing, that a deal had been done with Sussex police and the CPS, not to include any evidence that would upset the chances of the Crown obtaining a conviction. We know that Julian Dale was Eastbourne based and we know that the father of the jilted mother was a mason with the Tyrian Lodge in South Street, 100 yards away from Eastbourne police station at the top end of Grove Road.
We imagine that once these facts are known by Melanie Liebenberg, that she will have a tough time wrestling with her conscience, knowing that she helped Sussex police to craft the evidence in such blatant fashion. We hope then that she is not on the payroll and might have the decency as a human being to come forward and tell her story.
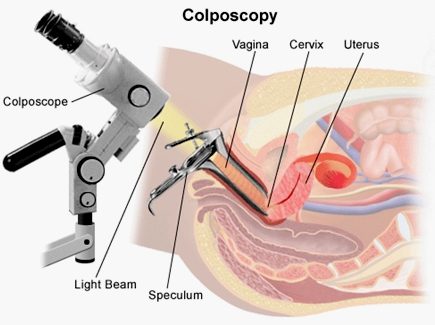
COLPOSCOPY
Colposcopy (Ancient Greek: κόλπος kolpos “hollow, womb, vagina” + skopos "look at") is a medical diagnostic procedure to examine an illuminated, magnified view of the cervix and the tissues of the vagina and vulva. A specialized colposcope equipped with a camera is used in examining and collecting evidence for victims claiming to have been raped or sexually assaulted. The technique should be gainfully employed and developed to identify the growing numbers of false allegations, so saving convictions based on testimony, that under the present system, is all that is needed to send a man down. Dame Butler Schloss is an advocate of enhancing our knowledge in this area and said as much in her remarks on the above RCPCH guidance.
Many premalignant lesions and malignant lesions in these areas have discernible characteristics which can be detected through the examination. It is done using a colposcope, which provides an enlarged view of the areas, allowing the colposcopist to visually distinguish normal from abnormal appearing tissue and take directed biopsies for further pathological examination.
The other use of colposcopy is to prevent cervical cancer by detecting precancerous lesions early and treating them. The procedure was developed in 1925 by the German physician Hans Hinselmann, with help from Helmut Wirths.
PROCEDURE
During the initial evaluation, a medical history is obtained, including gravidity (number of prior pregnancies), parity (number of prior deliveries), last menstrual period, contraception use, prior abnormal pap smear results, allergies, significant past medical history, other medications, prior cervical procedures, and smoking history. In some cases, a pregnancy test may be performed before the procedure. The procedure is fully described to the patient, questions are asked and answered, and the patient then signs a consent form.
After a complete examination, the colposcopist determines the areas with the highest degree of visible abnormality and may obtain biopsies from these areas using a long biopsy instrument, such as a punch forceps, SpiraBrush CX or SoftBiopsy. Most doctors and patients consider anesthesia unnecessary, save where multiple biopsy samples are to be taken - to decrease patient discomfort.
The results in sexual cases may have the same effect as a lie detector test, save that the physical examination and photographic record are more conclusive. If a girl has been raped, especially a young girl, there will be signs that prove penetration (rape) has taken place. This will be especially apparent in cases of non-consensual sex where no foreplay will mean no lubrication and so increased trauma in the form of tearing (scars) and bruising.
In the case below, apart from the fact that the girl was "tightly closed", there was also no signs of tearing of the fourchette, or other trauma associated with digital penetration (without foreplay = dry). The girl claimed regular assaults of this type that would have produced scars and the like in 83% of cases, but there were no scars, a finding which is clearly inconsistent with her claims.
A partial notch was found in the hymen, but it is now known that such findings are normal. Tears and the like in the hymen are full width if caused by trauma, leaving scar tissue, rather than partial (a smooth small indentation) as in naturally occurring features. This was not explained to the jury, who were left believing that there was no explanation for the 'notch' other than penetrative sex.
UNDERSTANDING
THE SEXUAL ABUSE EXAM - The "why"'s of the pediatric sex abuse
exam
or perianal lacerations
which is confirmed in the knee-chest position The authors warn that this classification "does not represent a consensus of medical experts regarding the classification of findings with respect to abuse."
In evaluating a report of sexual abuse, look for the following:
Berent W., "Case Study: Allegations of Abuse Created in a Single Interview", J. Am. Acad. Child. Adol. Psych. 36(7): 966-70, 1998. A baby-sitter videotaped her grilling of a child. Ultimately the child reported that the father killed a pink cow and a pink horse with a gun. "An elaborate, detailed allegation was created through the use of repetitive, suggestive questioning." Dr. Berent is at 1601 Twenty-Third Avenue South, Nashville TN 37212.
Levitt, C., Further Technical Considerations Regarding Conducting and Documenting the Child Sexual Abuse Examination", Child. Abuse Neg. 22(6): 567-586, 1998. Carolyn Levitt MD is director of the Midwest Children's Resource Center, Children's Health Care, 360 Sherman Street Suite 200 St Paul MN 55102.
Bays J, Chadwick D, The medical diagnosis of the sexually abused child. Child Abuse & Neglect 17: 91-110, 1993.
Britton H & Hansen K, "Sexual Abuse", Clin Ob Gyn 40(1): 26-239, 1997. First author is at 100 N Medical Drive Suite 3400, Salt Lake City, Utah, 84133. Lists:
Definitive for Sexual Abuse
prostatic acid
phosphatase" - Ed.)
Suspicious for Sexual Abuse
*
Nonspecific vaginitis (bacterial vaginosis)
Ed Friedlander MD
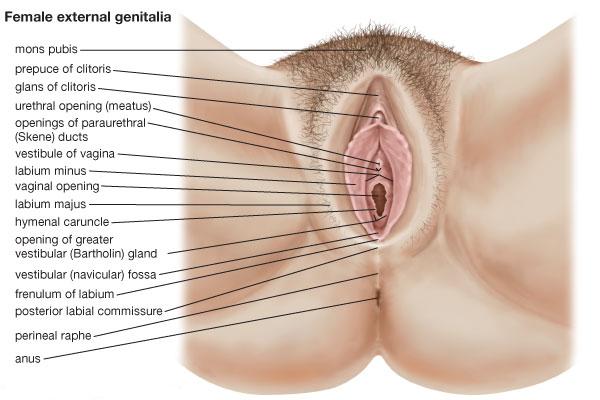
VIRGINITY TESTING
A virginity test is the practice and process of determining whether a female person is a virgin, i.e., whether she has never engaged in sexual intercourse. The test involves an inspection of a female's hymen, on the assumption that her hymen can only be torn as a result of sexual intercourse.
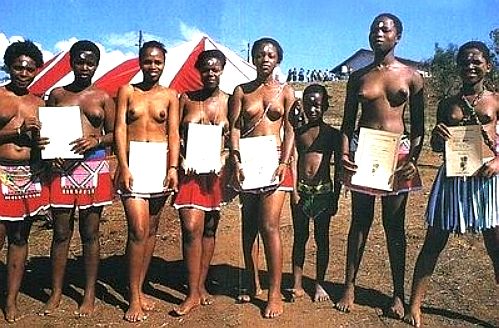
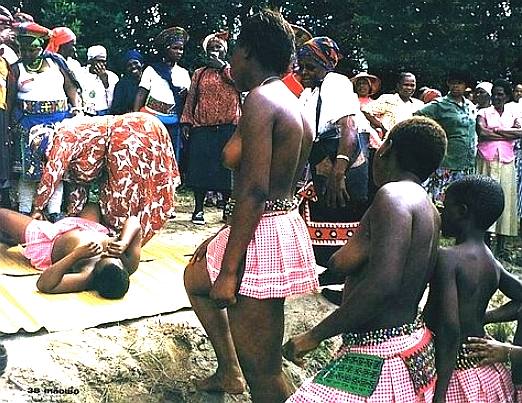
VIRGINITY TESTING - The Zulu tribes in South Africa invite girls to prove that they are virgins, reviving an African tradition seen by many as the answer to the scourge of AIDS. Bare-breasted teenagers wearing nothing but strings of beads and loincloths regularly submit to the ordeal of having a stranger check if their hymens are intact - then leaping for joy when the test confirms that they are still intact. Advocates say the revival of the rite is the most effective way to stop the spread of teenage pregnancies and the deadly HIV virus, believed to affect one in 10 South Africans. It's no different to young girls of 13 in the UK asking their doctor for the contraceptive pill, except that we give it to them. Who is doing things correctly here! Girls who pass get white stars pasted on their foreheads and a certificate confirming their virginity. Physical virginity tests were also reported in India from August 2009.
LINKS
http://www.pathguy.com/abuseexm.htm http://womenshealth.about.com/cs/cevicalconditions/a/colposcopy.htm http://en.wikipedia.org/wiki/Virginity_test http://en.wikipedia.org/wiki/Virginity_fraud http://www.nhs.uk/Conditions/colposcopy/Pages/Introduction.aspx Virginity tests zulu south africa
THE ULTIMATE RAPE - ANATOMY OF A STITCH UP - FLOW CHART - REAL LIFE INJUSTICE
In a case where sexual assault is claimed, it is vital for investigators to act quickly to prevent potential witnesses from rehearsing and developing a version of a false claim. The investigators in this case allowed the claimant two weeks to rehearse a story, all the while she was obtaining feedback from social services and friends as to what to say such that it might be acceptable (believed). Coaching or rehearsing a story is of course illegal. Clearly, in this case coaching is a major feature. SOCAP procedures are designed to prevent coaching by obtaining a statement the moment an allegation is made. By this means false allegations may be revealed by preventing changes to a story that repair obvious lies that a defence will be able to disprove. We are following this Sussex case and will report news as it happens.
Many policemen are Masons, there is no denying this. This can lead to corruption at high levels, where fellow Masons, members of the public, might obtain favours, as in charges being dropped, or charges brought against someone, as examples. The law is quite often used incorrectly (illegally) to further the objectives of private causes in organized fashion. But who is there to investigate? Since many, if not most high ranking officers are Masons, and their siblings, even if not masons, in whichever force, even an outside force is unlikely to identify an officer who will make any effort to investigate a fellow officer. It's a club, for a favoured few in positions of trust - and there is no real complaint system that bears scrutiny.
On this site you will find information of corruption in all walks of life, and those targeted who may have brought the actions of council officers to the public's attention, such as Wealden Action Group members, on the instigation of known Masons, councillors, or planning officers, many of which are themselves Masons.
Every regional Police Force has its own website which contains information and advice about police activity in the area it serves. You can select your local force, or the force for another region below: However, you will not find any information as to how to report planning crime. If you do report a planning crime, the force you have contacted will write back explaining it is a civil matter, despite the criminal sanctions in the Town & Country Planning Act as amended by the Planning & Compensation Act. If you really push for a crime to be logged, they will tell you they do not have the resources and to take out a civil action. Clearly, this is a crime in itself as in R v Dytham and R v Bowden - failing to perform one's duty to uphold the law. Please also see the Police Act and Code of Conduct elsewhere on this site. Just click the links.
It appears the UK Police Service works alongside a number of Government organisations, masquerading as independents, to stifle planning crime and suppress public outcry. The best thing you can do if you recognise any of the symptoms, is to lobby your Member of Parliament for a change in the law. The Ombudsman, District Auditor and Office for the Supervision of Solicitors are all their to preserve the status quo, regardless of the ongoing injustice:-
HOME OFFICE LINKS POLICE ASSOCIATIONS AND FEDERATION LINKS POLICE AUTHORITIES NATIONAL SERVICES LINKS
LINKS & REFERENCE
The Guardian US news 2015 June 23 FBI evidence single hair Kirk Odom https://www.documentcloud.org/documents/2081513-microscopy-of-hair.html https://www.ncjrs.gov/pdffiles1/nij/grants/228091.pdf http://www.theguardian.com/us-news/2015/jun/23/fbi-evidence-single-hair-kirk-odom http://twitter.com/edpilkington http://www.telegraph.co.uk/Romford-and-Eastbourne-hospitals-dragged-in-to-NHS-care-scandal.html www.drfosterhealth.co.uk/consultant-guide/Dr-Melanie-Anne-Liebenberg
This site is protected under Article10 of the European Convention on Human Rights and Fundamental Freedoms.
FAIR USE NOTICE
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, scientific, and social justice issues, etc. We believe this constitutes a 'fair use' of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||