|
THE PHYSICAL SIGNS OF
CHILD SEXUAL ABUSE
An evidence-based review and guidance for best practice
This handbook is a revision of the 1997 Royal College of Physicians publication 'Physical Signs of Sexual Abuse in Children'. Based on the best available evidence, it has been produced by the Royal College of Paediatrics and Child Health in collaboration with the Royal College of Physicians of London and its Faculty of Forensic and Legal Medicine.
The review focuses on evidence for the physical signs of child sexual abuse (CSA) in the following areas: female genitalia; male genitalia; anal signs; oral signs; and sexually transmitted infections.
The literature search has been updated and an interim statement summarising the findings is available to download: CSA Interim statement (PDF,53KB,6 pages)
A full update will be undertaken in 2012/2013 and a second edition published in late 2013. This will include new sections on healing, thermal injuries and accidental/non-intentional injuries.
Please note: The Royal College of Paediatrics and Child Health, Association of Chief Police Officers and Faculty of Forensic Medicine have recently updated the document 'Guidance for best practice for the management of intimate images that may become evidence in court'.
Get a copy of the CSA Publication
The publication is available free of charge to all designated and named doctors (email:
clinical.standards@rcpch.ac.uk), and may otherwise be purchased for delivery.
The review may be ordered through the Lavenham Group. The charges include shipping and handling and are as follows:
FREE to designated and named doctors
Delivery within the UK: £31.06
Delivery to Europe: £40.06
Delivery to the rest of the world: £46.06
Contact
Lavenham Group plc
Arbons House
47 Water Street
Lavenham
Suffolk
CO10 9RN
Telephone 01787 249 199 / Fax 01787 248 267
For further information:
Website: http://lpl-uk.com/index.php
Email Lavenham Group: rcpch@lavenhamgroup.co.uk
Cheques may be made payable to 'Lavenham Group plc' and posted to the address above.
Last published on 18 April 2013
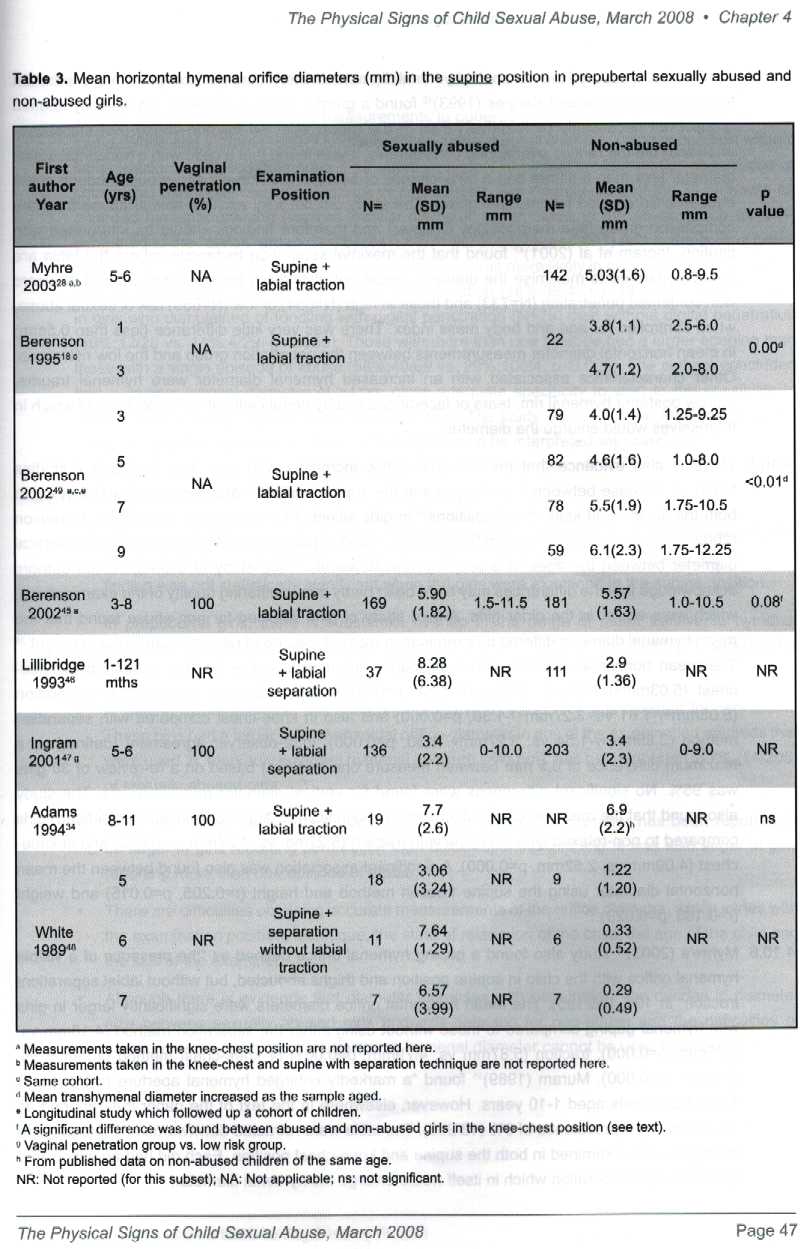
According
to the RCPCH guidance on page 46 (4.10.3) Two studies compared the
measurements of horizontal hymenal diameter in sexually abused girls and
girls selected for non-abuse in the supine position with labial
traction. Table 3 (above) presents horizontal measurements in the supine
position and illustrates the considerable overlap in ranges. In a case
control study, Berenson (2002) found that girls with a history of
digital or penile vaginal penetration (N=189) had a larger mean
tranverse hymenal diameter compared to non-abused girls (N=197) when
examined in the knee-chest position (5.6+-1.8mm, range 2.0-10.25mm vs.
4.6+/-1.9, range 1.0-10.5mm, p<0.01_ but not in the supine position
(reported in Table3).
Controlling
for race and age, abused girls were 2.4 times more likely that
non-abused girls to have a horizontal hymenal diameter over 6.5mm in the
knee chest position, (95% Cl: 1.4mm-4.2mm) but with low sensitivity if
29% and specificity of 86%.
(4.10.4)
Two studies measured the horizontal diameter in the supine position with
labial separation technique. Lillybridge and Kappes (1993) found a
greater mean diameter in the sexually abused group ("not
necessarily penetrative") than in the group selected for non-abuse.
It was found that a child with a horizontal orifice diameter less than
6.94mm had a 99% chance of being in the non-abused group although some
abused children also fell into this group.
From
the above one might expect to have noted a hymenal variation from the
normal if the subject "GG" had been penetrated as claimed. But
of equal importance is the fact that there were no transections, angular
clefts or tears as one might expect from the more damaging repeated
digital penetrations claimed. This is an interesting case that may
advance the science of forensic medicine such as to detect falsehoods at
an early stage - so saving the state considerable sums, that might be
better spent prosecution those where there is evidence to support abuse
claims.
It is important
when constructing a jigsaw puzzle, to have all the pieces. For example,
the examiner, Doctor Melanie Liebenberg, did not know that there had been heated exchanges between the
defendant and her mother and that he'd recently called off an engagement. None of the Class
3-4 signs were present, as one might have expected if as claimed, the girl
had been regularly penetrated. The trial judge,
Cedric Joseph, told the jury this might
have been on 40 occasions.
One can but imagine
the state of a vagina if assaulted 40 times with no foreplay. It would
not be intact for sure. NOTE: None of the above was available for a
trial held just weeks before publication in March of 2008.
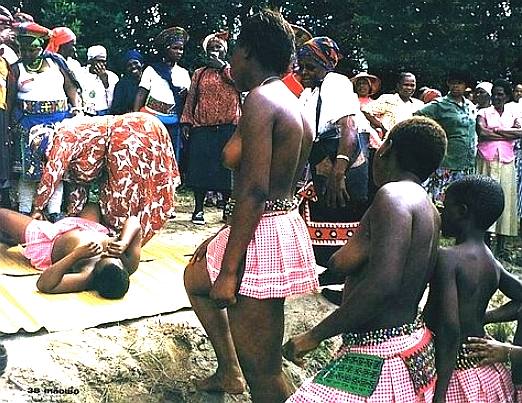
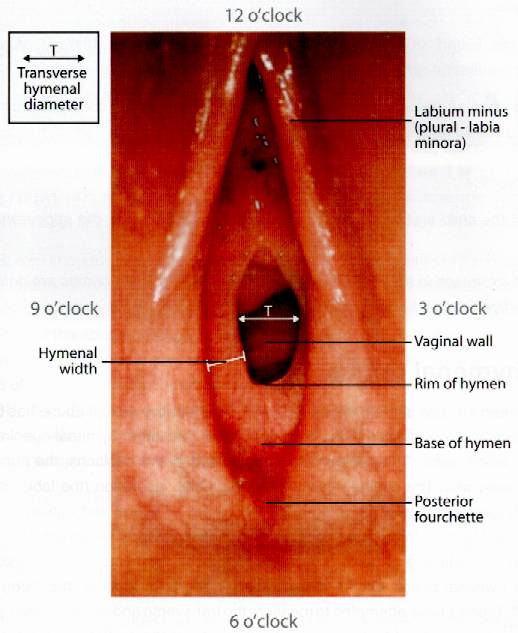
If
tribes in Africa can tell if a girl is a virgin or not, how is it that in
Eastbourne, a doctor with an array of modern instruments cannot. Dr
Liebenberg failed to mention to the jury that none of the expected
lacerations, transections and/or healed scars to the fossa or posterior
fourchette - or angular clefts or tears, or labial adhesions of the hymen
were present. She might have mentioned that the absense of any and all of
these signs, given the claimed regularity of abuse, was not consistent
with the allegations. Dr Liebenberg could have mentioned that had any of
these signs been in evidence, that would have been either definitive proof
of sexual abuse or at best highly suspicious circumstances. But, as we
stress - none
of these were present and the jury had a right to know that before
sending a man to prison.
All
of the above needs to be read in the context of a diary that eliminates
opportunity in at least one location, thus undermining the credibility
of the Crown's witnesses.
ANATOMY
OF A STITCH UP - FLOW CHART
|
|
ALLEGATION
SEXUAL ASSAULT 2006
follows
acrimonious family break up
|
|
|
|
|
|
|
|
|
|
TEACHER
loses
her note of original version of events
|
FRIENDS
report
their version of gossip
|
SOCIAL
WORKERS
failure
to investigate claims
|
|
|
|
|
|
|
|
|
|
CHILD
PROTECTION UNIT (Breaches SOCAP procedures)
|
|
|
|
|
|
|
|
|
|
2nd
OFFICER
|
|
INVESTIGATING
OFFICER
failure
to secure crime scene evidence
|
|
3rd
OFFICER
|
|
|
|
|
|
|
|
|
|
PATIENTS
DOCTOR
|
MEDICAL
EXAMINATION
uses
out of date forensic guidance in a controversial area of science
- defence barrister fails to challenge
|
PSYCHOLOGIST
|
|
|
|
|
|
|
|
|
|
|
|
DEFENDANT
CHARGED
Eastbourne
Magistrates Court
|
|
|
|
|
|
|
|
|
|
|
|
|
CPS
WITNESSES
Barrister
fails to apply to question claimant
|
|
|
|
|
|
|
|
|
|
|
|
FRIENDS
|
DEFENCE
WITNESSES
Barrister
fails to interview any of 17 witnesses for defence
|
FAMILY
|
|
|
|
|
|
|
|
|
|
|
|
MEDICAL
EVIDENCE
Barrister
fails to challenge medical evidence even after Lewes Crown Court
Judge tells him to get on to it.
|
|
|
|
|
|
| |
|
|
|
|
|
SX
POLICE
Refuse
to return defence computer evidence or to confirm nothing
untoward on computers. Court eventually force Police to return.
|
|
|
|
|
|
|
|
|
|
|
|
|
TRIAL
COURT FEB 2008
Hove
Crown Court - conservative venue with high conviction rate
|
|
|
|
|
|
| |
|
|
|
SOLICITOR
Cramp
& Co
|
BARRISTER
Sussex
Chambers
|
JURY
SWORN IN
|
BARRISTER
|
SOLICITOR
|
|
|
|
|
|
|
|
|
ARGUS
|
BECKETT
GROUP
|
PRESS
Publish
mid-trail in violation of Court Order to preserve fair hearing -
contempt of Court. Trial Judge, Cedric Joseph, fails to remedy.
|
SX
EXPRESS
|
KENT
& SX COURIER
|
|
|
|
|
|
|
|
|
|
|
JUDGES
SUMMING UP
|
|
|
|
|
Misdirects
Jury on vital diary evidence and asks them to decide medical
issues for which no juror is qualified
|
|
|
|
|
|
|
|
|
|
|
|
VERDICT
FEB 6 2008
A
guilty verdict is returned
|
|
|
|
|
JUSTICE
|
|
|
INJUSTICE
|
|
|
|
APPEAL
PROCESS BEGUN MAY 2008
|
|
|
APPEAL
SOLICITOR
Stuart
Grace & Co |
| |
1st
APPEAL BARRISTER
Michael
Harrison |
|
|
|
APPLICATION
TO COURT OF APPEAL requesting transcript of medical testimony |
|
|
|
|
|
| |
|
|
|
|
Her
Majestys's Court Service (HMCS) - refused transcript = abuse of
process Appeal barrister unable to perfect grounds |
|
|
|
|
| |
|
|
|
|
|
SINGLE
JUDGE
Sir
Christopher Holland - refuses leave and initials box -
compounding abuse of process
|
|
|
|
|
|
|
|
|
|
|
|
|
APPLICATION
TO ECHR May 2009
28536/09
|
|
|
|
|
|
|
|
|
|
|
|
APPLICATION
TO CCRC December 2009
In
England once leave to appeal is refused, there is no other
appeal process save via the Criminal Cases Review Commission
|
|
|
|
|
|
|
|
|
|
|
|
LEGAL
AID APP FUNDING 2010
|
|
|
|
|
|
| |
|
|
|
SOLICITOR
(CCRC)
Wells
Burcombe & Co |
| |
BARRISTER
(CCRC)
Dominic
Chandler |
|
|
|
CCRC
2010
Provisionally
refuse application. |
|
|
|
|
|
| |
|
|
|
|
|
CCRC
2010
Freedom
of Information request reveals new medical guidance exists which
the CCRC had neglected to mention |
|
|
|
|
|
|
|
|
|
|
|
|
LEGAL
AID APP FUNDING 2011
For
report as to natural marks and virginity reference RCPCH
guidance March 2008 - one month after trial.
|
|
|
|
|
|
| |
|
|
|
SOLICITOR
Ross
Simon & Co
Chizzy
Nsofor |
| |
BARRISTER
Lucy
Corrin |
|
|
|
|
|
|
|
|
|
|
CCRC
2011
Obtain
limited forensic Report as to naturally occurring marks.
|
|
|
|
|
|
| |
|
|
|
|
|
CCRC
2012
Admit
medical evidence to Jury misleading - but refuse to investigate virginity
issue, diary misdirection or provide transcript they have
obtained as to revelation of diary mid-trial. |
|
|
|
|
|
|
|
|
|
|
|
|
LEGAL
AID APP FUNDING 2012
To
seek a Judicial Review of CCRC's refusal to investigate
inconsistencies in evidence as above.
|
|
|
|
|
|
| |
|
|
|
SOLICITORS
JUDICIAL REVIEW
David
Wells & Siobhan Tipper |
| |
BARRISTER
Stephen
Field |
|
|
|
| |
|
|
|
|
|
HIGH
COURT (ADMIN) 2013
Refuse
leave for a Judicial Review
|
|
|
|
|
|
| |
|
|
|
|
|
LEGAL
AID REFUSE FUNDING
To
Appeal to the Appeal or Supreme Court
|
|
|
|
|
|
| |
|
|
|
ECHR
Fresh
Application having exhausted possible domestic remedies |
|
|
|
|
|
| |
|
|
In
a case where sexual assault is claimed, it is vital for investigators to
act quickly to prevent potential witnesses from rehearsing and developing
a version of a false claim. The investigators in this case allowed the
claimant two weeks to rehearse a story, all the while she was obtaining
feedback from social services and friends as to what to say such that it
might be acceptable (believed). Coaching or rehearsing a story is of
course illegal. Clearly, in this case coaching is a major feature. SOCAP
procedures are designed to prevent coaching by obtaining a statement the
moment an allegation is made. By this means false allegations may be
revealed by preventing changes to a story that repair obvious lies that a
defence will be able to disprove.
Clearly,
in allowing 2 weeks for the claimant to speak with friends and social
services, the Sussex Police were negligent in this case, depriving the
defence of a valuable record of changes in the story as the allegation was
developed. Was this simple negligence or criminal negligence? The CPS
knew this was going on and used it to their advantage.
RIGHT
OF REPLY
If
any person who wishes to refute the facts as published herein, we would
like to hear from you. A failure to respond to this invitation will be
taken as deemed acceptance.
CSA Reviewers:
Dr Maysoon Aldoori, Consultant Paediatrician, Dumfermline and West Fife CHP, Scotland
Dr Amanda Bennett, Consultant Community Paediatrician, Alder Hey Children's Hospital,
Dr Christine Bowman, Consultant Physician in GU Medicine, Sheffield Teaching hospitals
Dr Maria Bredow, Consultant Paediatrician, United Bristol Healthcare NHS Trust
Miss Frances Corrigall, Researcher, RCPCH, London (Jan 07-Jul 07)
Dr Margaret Crawford, Consultant Paediatrician, United Lincolnshire Hospitals Trust
Dr Dominic Croft, Consultant Community Paediatrician, Danestrete Centre, Stevenage
Dr Emma Curtis, Consultant Community Paediatrician, Adelaide and Meath Hospital,
Dr Geoff Debelle, Consultant Community Paediatrician, Birmingham Children's Hospital NHS Foundation Trust
Dr Juliet Farquhar, Specialist Registrar, Yorkhill Hospital, Glasgow
Miss Lavinia Ferrante Ruffano, Researcher, RCPCH, London (Jan 07-Jul 07)
Dr Fiona Finlay, Consultant Community Paediatrician, Bath & North East Somerset PCT
Dr Greta Forster, Lead Clinician, Haven Whitechapel and Consultant Physician in
Dr Sara Ghulam, Consultant Community Paediatrician, East Kent Hospitals NHS Trust
Dr Carys Graham, Consultant Community Paediatrician, National Public Health Service for
Mrs Linda Haines, Head of Research, RCPCH, London
Dr Julia Hale, Consultant Paediatrician, Bexley Care Trust
Dr Chris Hobbs, Consultant Paediatrician, Leeds Teaching Hospitals NHS Trust, Leeds
Dr Elaine Lewis, Consultant Community Paediatrician, Addenbrooke's Hospital, Cambridge
Dr Anne Livesey, Consultant Community Paediatrician, Alexandra Hospital for Sick Children Brighton
Dr Lindsay Logie, Consultant Paediatrician, Royal Hospital for Sick children, Edinburgh
Dr Jane Macdonell, Consultant Paediatrician, Borders General Hospital, Scotland
Dr Una MacFadyen, Consultant Paediatrician, Stirling
Dr Alison Maddocks, Consultant Paediatrician, National Public Health Service for Wales
Dr Jacqueline Mok, Consultant Paediatrician, Department of Community Child Health,
Dr Alison Mott, Consultant Paediatrician, Cardiff & Vale NHS Trust, Cardiff
Dr Olusoji Olakanpo, Researcher, RCPCH (Apr 06-Feb 07)
Dr Elizabeth Penny, Consultant Community Paediatrician, Cardiff & Vale NHS Trust, Cardiff
Dr Mary Pillai, Consultant Obstetrician Gynaecologist, Cheltenham General Hospital
Dr Katia Prime, Locum Consultant Physician in Genitourinary Medicine
Miss Rita Ranmal, Clinical Effectiveness Co-ordinator, RCPCH, London
Dr Alicia Rawlinson, Consultant Community Paediatrician, Royal Gwent Hospital
Dr Jane Ritchie, Consultant Paediatrician, Kent and Medway NHS and Social Care
Dr Deborah Rogers, Faculty of Forensic and Legal Medicine, London
Dr Karen Rogstad, Consultant Physician in Genitourinary Medicine/Honorary Senior
Dr Jane Schulte, Consultant Community Paediatrician, North Bristol NHS Trust
Dr Ruth Skelton, Consultant Paediatrician, Bradford Hospitals NHS Trust
Dr Hilary Smith, Consultant in Community Child Health, Royal Manchester Children's Hospital
Dr Sally Stucke, Consultant Community Paediatrician, Herefordshire Primary Care Trust
Dr Amanda Thomas, Consultant Paediatrician, Leeds Primary Care Trust, Leeds.
Dr Catherine Tooley, Cambridge
Dr Hazel Walter, Forensic Physician, Herefordshire
Dr Jane Watkeys, Consultant Community Paediatrician, Swansea NHS Trust
Dr Dawn Wilkinson, Consultant Genitourinary Medicine, Jefferiss Wing Centre for Sexual
Dr Olwen Williams, Consultant Physician in Genitourinary Medicine, Wrexham Maelor
Last published on 15 June 2011
LINKS
http://www.rcpch.ac.uk/child-protection/publications/child-protection-publications
http://www.rcpch.ac.uk/GuidanceonIntimateImages30JUNE2010.pdf

His
barrister didn't challenge the so-called scientific evidence produced at
trial. He should have. It was junk science. You'll have to wait for the
subjects appeals in the ECHR to conclude before this book is published.
Maybe then we'll see an official version in 2016/2017? European appeals
take 4 years on average, from date of lodge. But first you have to exhaust
any domestic remedy. He has finally, as of February 2013. A claim was
lodged in July of 2013.
|
FAIR
USE NOTICE
This
site contains copyrighted material the use of which has not always been
specifically authorized by the copyright owner. We are making such
material available in our efforts to advance understanding of
environmental, political, human rights, economic, scientific, and social
justice issues, etc. We believe this constitutes a 'fair use' of any such
copyrighted material as provided for in section 107 of the US Copyright
Law. In accordance with Title 17 U.S.C. Section 107, the material on this
site is distributed without profit to those who have expressed a prior
interest in receiving the included information for research and
educational purposes.
|
|
This
site is protected under Article10
of the European Convention on Human
Rights and Fundamental Freedoms. |
|